- High Intensity Focused Ultrasound (HIFU)
(i) HIFU is a relatively new treatment modality for benign uterine tumours.
(ii) It is a technology which involves focusing beams of ultrasound wave to one point, typically a small volume of 5 mm in diameter. The intention is to raise the temperature to above 60C for one second or longer in order to cause tissue necrosis. By moving this focus to different parts of the tumour, the majority of the tumour can be destroyed.
(iii) During the ablation process, the HIFU beam has to be targeted and monitored under image guidance either by MRI or ultrasound.
(iv) The application of this technique under ultrasound guidance (USgHIFU) as treatment of uterine fibroid has been reported in Mainland China since 2002. Since then, USgHIFU has been further developed and is now considered as one of the alternative treatments for fibroids apart from surgery in many parts of China.
(iv) The application of this technique under ultrasound guidance (USgHIFU) as treatment of uterine fibroid has been reported in Mainland China since 2002. Since then, USgHIFU has been further developed and is now considered as one of the alternative treatments for fibroids apart from surgery in many parts of China.
(v) The success rate of HIFU in treatment of fibroid(s) depends on the percentage of the fibroid being destroyed. In general, the fibroid shrinks by 45% at 3 months after treatment and this increases to 60% by 6 months. It is expected that 50% of patients will have improvement of symptoms at 3 months and this will increase to 90% at 6 months.
(vi) HIFU is in general a safe procedure under expertise team. Operative risks are uncommon but can occur. They include skin burn, acute urinary retention, pain at lower spine or legs, nerve and bowel injury.
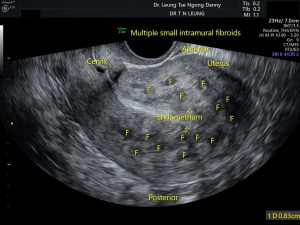
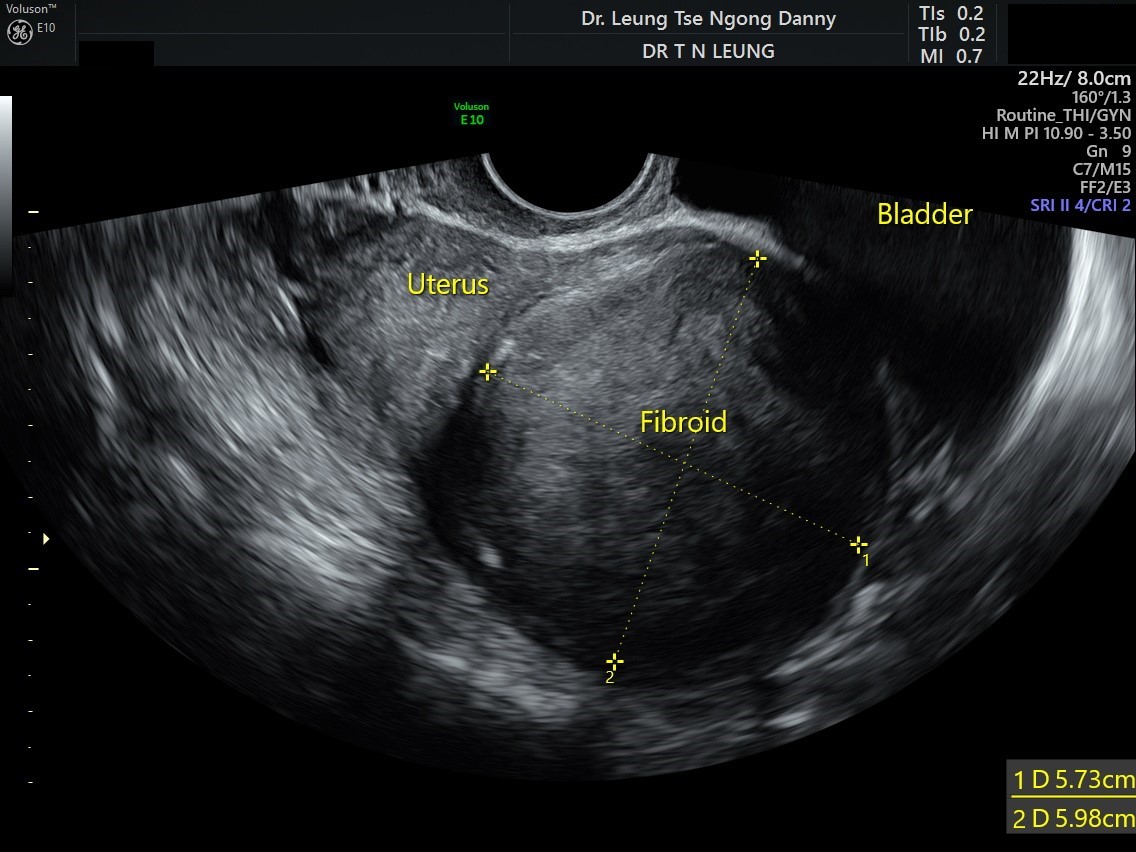
(vii) Not all women with uterine fibroids will benefit from HIFU treatment. For the location of some fibroids, HIFU may not be possible or can be dangerous Careful pre-operative assessment by ultrasound and MRI is very important for selection of suitable women who will likely benefit from it.