Tissues from the lining of the uterus has migrated to grow within the uterine muscle wall
Adenomyosis tissues are influenced by the female hormones and will have periodic bleeding within the muscle wall, causing menstrual pain. The growth of these adenomyosis tissues will also thicken the uterine wall
The lesions can also migrate to different parts of the uterine wall, enlarging the entire uterus. With an enlarged uterus, the period will be heavy
Sometimes the adenomyosis tissues can be confined to one part of the uterine wall, like a localized tumour. It is then called an “adenomyoma”
What are the symptoms of adenomyosis?
Some do not have symptoms, especially if the lesions are small
Painful period (dysmenorrhea), which may interfere with daily life
Heavy menstrual bleeding, which can lead to anaemia
How is adenomyosis diagnosed?
Ultrasound – more common and less expensive
Magnetic Resonance Imaging (MRI) – more accurate in making diagnosis and localizing the adenomyosis lesions. Much clearer images compared with ultrasound, but a more expensive test
What medications are available for adenomyosis?
Painkillers, like Paracetamol and Non-steroidal anti-inflammatory drugs (such as Ibuprofen)
Medication to reducing menstrual loss
Hormonal medicines, including oral contraceptive pills, oral progestogen pills, birth control injection, and progestogen-containing intrauterine contraceptive device (Mirena)
What are the surgical options for adenomyosis?
Hysterectomy – Since the boundary between adenomyosis and the adjacent normal uterine muscle is generally not obvious, it is difficult to excise the adenomyosis selectively. Hence, the entire uterus is usually removed to eradicate the pathology
HIFU (High Intensity Focused Ultrasound) – Special machine to emit focused high energy at the lesions to ablate the pathology
Adenomyosis – Full article
1. What is adenomyosis?
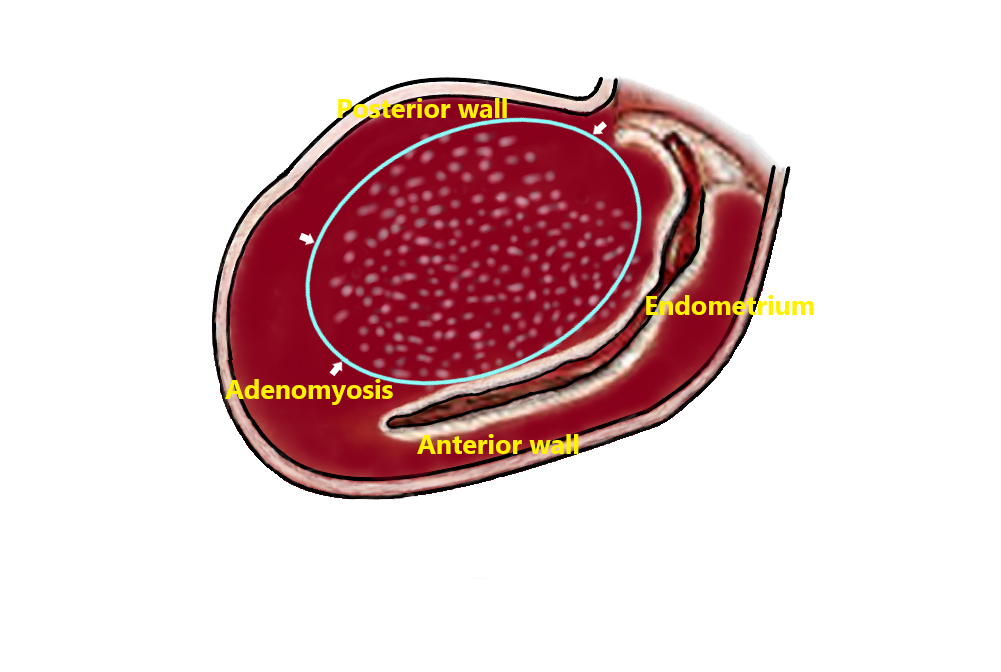
Adenomyosis is a benign gynecological disease in which tissues that originally grow in the lining of the uterus (endometrium), invade and grow within the uterine muscle wall. Like the glands of the endometrium, these adenomyosis tissues are affected by female hormones and will have periodic bleeding within the muscle wall. This causes pain during the menstrual period (dysmenorrhea).
The growth of these adenomyosis tissues will also cause thickening of the uterine muscle wall. Sometimes the lesions can spread to different parts of the uterine wall, enlarging the entire uterus. With a big uterus, the menstrual bleeding can be heavy.
2. The difference between ‘adenomyoma’ and ‘fibroid’
Sometimes the adenomyosis tissues can be confined to one part of the uterine wall, like a localized tumour. It is then called an ‘adenomyoma’.
It is different from uterine fibroid, which is called ‘leiomyoma’ in medical term. Fibroid is a benign tumour made up of muscles and fibrous tissue and grows in the wall of the uterus. There is a ‘capsule-like’ structure surrounding a fibroid, separating it from the neighbouring normal uterine muscle.
Adenomyoma, on the other hand, is composed of endometrial tissue and secretory glandular stroma, and there is no capsule separating the lesion from the surrounding normal uterine muscle.
3. Symptoms of adenomyosis
Women with adenomyosis can have no symptoms at all, especially when the lesions are small. The most common symptoms are painful period (dysmenorrhoea) and heavy menstruation (menorrhagia), and the severity varies from person to person. For severe cases, it can be extremely debilitating because the pain can affect the daily living and social life, whereas the menorrhagia can cause severe anaemia. For those with very much enlarged uterus, a mass might be noted at the lower tummy.
4. Diagnosis of adenomyosis
The diagnosis of adenomyosis relies primarily on the use of ultrasound and/ or magnetic resonance imaging (MRI).
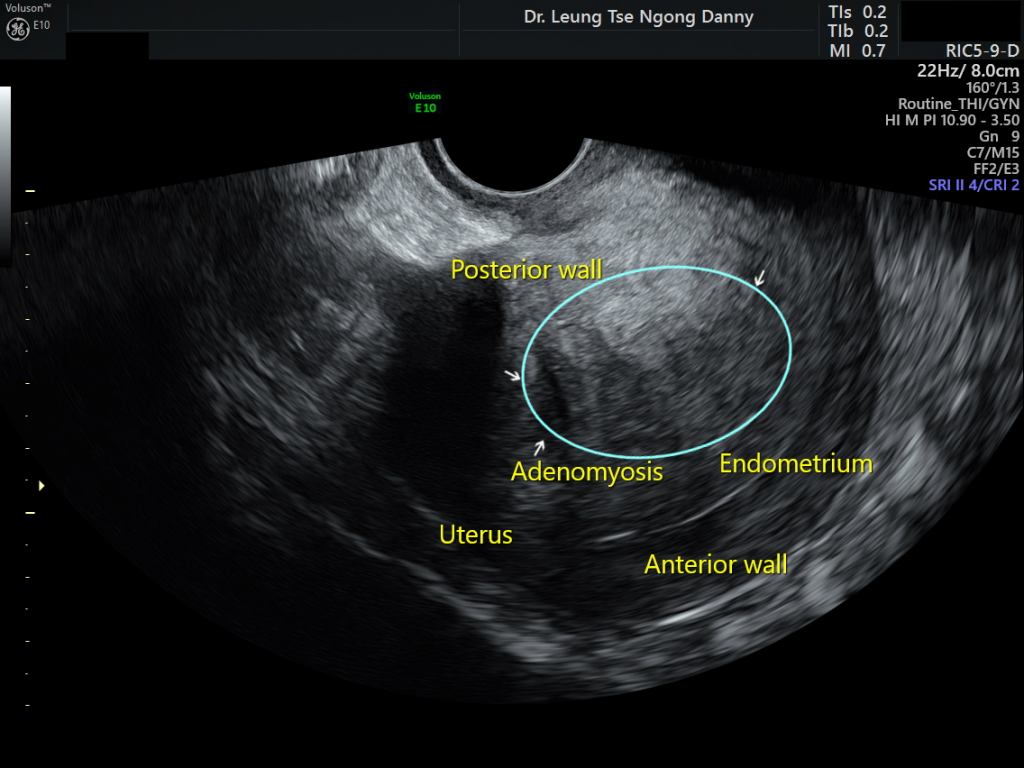
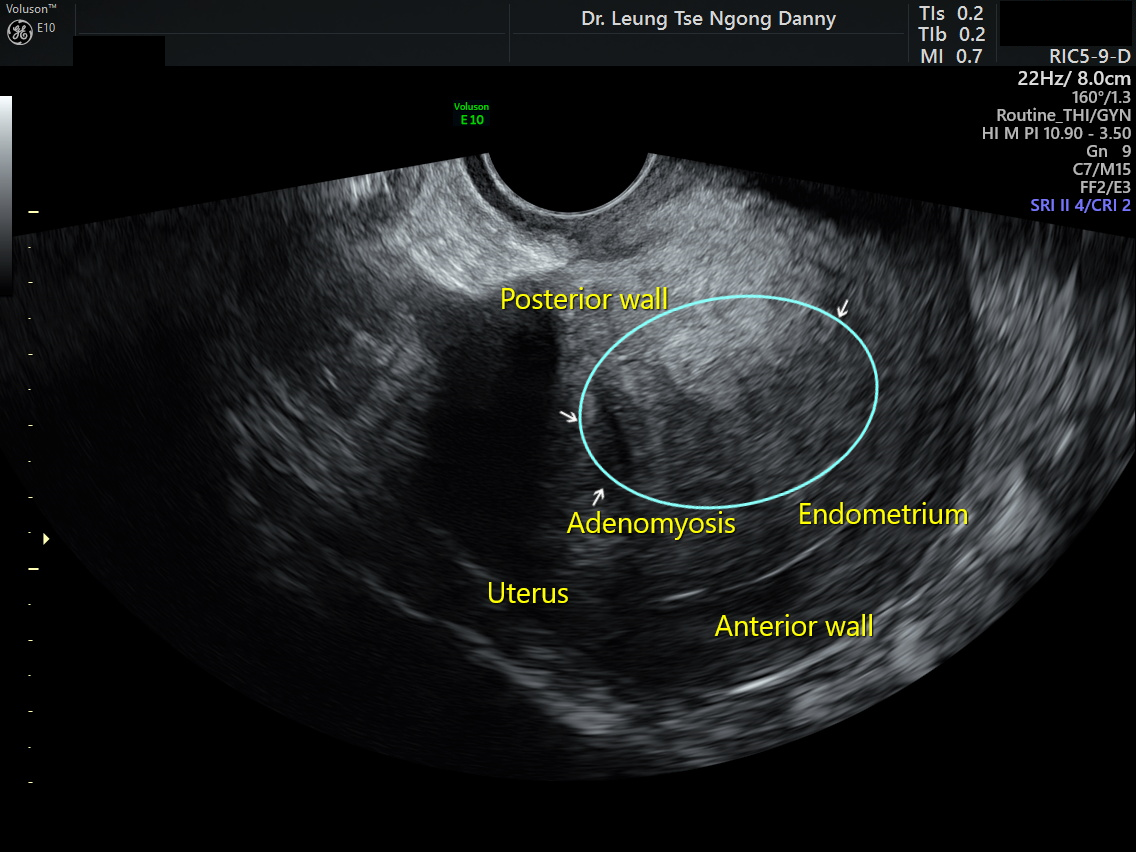
Ultrasound examination of the pelvis is a common and relatively inexpensive method in clinical practice. Ultrasound features of adenomyosis may include the followings:
(i) the entire uterus is globularly enlarged
(ii) the affected uterine wall is thickened
(iii) small cystic spaces within the muscle wall
(iv) small bright spots areas
(v) linear stripes or fan-shaped shadowing at the affected area
adenomyosis (ultrasound)
adenomyosis
MRI is more accurate in diagnosing and locating adenomyosis than ultrasound. The images are much clearer, allowing better demarcation of the extent of the lesions. However, it is more expensive than ultrasound.
Adenomyoma (MRI)
5. Treatment of adenomyosis
Asymptomatic patients do not need any treatment
If symptoms are mild, try medication to control symptoms e.g. painkillers such as paracetamol or nonsteroidal anti-inflammatory medication (NSAID e.g. Ibruprofen) for dysmenorrhea; and haemostatic medication during menstruation to reduce menstrual blood loss
If symptoms are severe, the above medication will usually fail. Hormonal medication can be tried. It includes oral contraceptives, oral progestogen pills, birth control injections, and progestogen-containing intrauterine contraceptive device (Mirena).
Some do not respond to NSAID and hormonal medication, especially those with large lesions. If medical treatment is ineffective, surgical intervention is indicated.
(i) Adenomyomectomy
Ideally, the lesions should be resected to remove the pathology. However, it is technically rather difficult because the adenomyoma was not surrounded by a capsule and hence the boundary between the lesions and the neighbouring normal uterine muscle is not distinct. The excision could also be incomplete as adenomyosis can be very diffusely located in the muscle wall. Attempts to excise adenomyoma using open laparotomy or laparoscopic approach have been reported in some centres. However, at the time of writing of this article, this surgical procedure is not widely available or commonly practised.
(ii) Hysterectomy
As the selective excision of the adenomyoma is difficult as stated above, removal of the entire uterus, a procedure called ‘hysterectomy’ is usually the surgical option. This is suitable for women with very severe symptoms and no fertility wishes.
(iii) HIFU
Another feasible treatment option is HIFU (High Intensity Focused Ultrasound). It is a technology which involves focusing beams of ultrasound wave to one point, typically a small volume of 5 mm in diameter. The intention is to raise the temperature to above 60C for one second or longer in order to cause tissue necrosis. By moving this focus to different parts of the tumour, the majority of the tumour can be destroyed.
HIFU has been investigated for treatment of adenomyosis since 2007. Based on the evidence in the medical literature, HIFU helps to reduce the symptoms of dysmenorrhea and menstrual blood loss by an average of 50% to 70% at 12 months after the procedure. Another benefit of HIFU is that the uterus and hence the fertility can be preserved. Pregnancies after HIFU ablation of adenomyoma have also been reported in the literature.
Not all women with adenomyosis/ adenomyoma are suitable for HIFU treatment. For the location of some adenomyoma, HIFU ablation may not be possible or can be dangerous. Careful pre-operative assessment by ultrasound and MRI is very important for selection of suitable women who will likely benefit from the treatment modality. In addition, because the uterus is preserved, even if the lesion is ablated, there is a chance of recurrence of adenomyosis elsewhere in the uterus in a long run.
This article is contributed by Dr. T.N. Danny Leung