1. What is cervical incompetence?
- Cervical incompetence is a condition where the cervix has functional disability that fails to maintain the pregnancy to term.
2. What is the typical presentation?
- The typical presentation is the presence of significant cervical dilatation without uterine contraction in the 2nd trimester. It usually occurs at around 18-24 weeks of gestation when the growing pressure of the pregnancy is too much for the cervix to hold, leading to a rapid miscarriage. It is commonly accompanied by a lot of mucoid vaginal discharge prior to the event of delivery. When cervical dilatation is detected, the amniotic membrane might have already herniated through the external exit (external os) of the cervix. The delivery is typically very quick with minimal contraction pain.
- However, it is also postulated that cervical incompetence might predispose to ascending infection (infection of the placenta and amniotic membrane). The subsequent inflammatory response to the intrauterine infection may lead to miscarriage, preterm pre-labour rupture of membranes, preterm labour and delivery. The clinical course will be different from the typical presentation of silent cervical dilatation and miscarriage.
3. Difficulty in diagnosis
- The diagnosis is straightforward in the presence of a typical presentation in the previous pregnancy. However, if the clinical course of a mid-trimester miscarriage or very early preterm birth (< 34 weeks of gestation) is not as typical, it is difficult to determine whether there is an element of cervical incompetence as the predisposing factor.
- It has been suggested that women with such atypical presentation can have an assessment of the cervix in the non-pregnant state. Easy passage of a sized 8 Hegar dilator through the cervix or an imaging technique called cervico-hysterogram showing dilatation of the cervical canal with loss of the internal os are two traditionally used criteria for the diagnosis of cervical incompetence. However, these tests are not subjected to validation studies.
4. Cervical length and incompetence
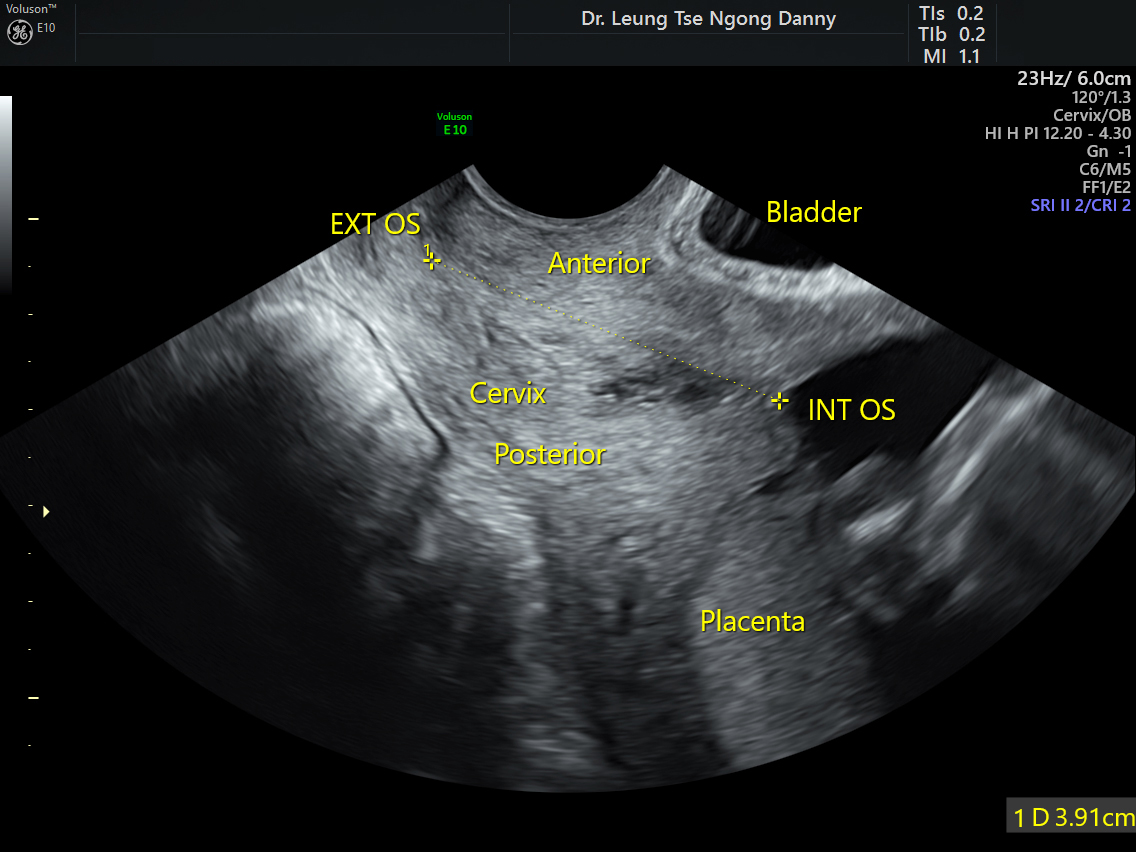
- During pregnancy, the cervical length in the second trimester measured by transvaginal ultrasound is known to be a marker for preterm birth. The shorter the cervix, the higher the risks for preterm delivery < 34 weeks of gestation. The mean cervical length at 20-22 weeks of gestation is around 35 mm. Different criteria of ‘short cervix’ have been used in different studies and units, including 15mm, 20mm and 25mm.
-

- Normal cervical length
-

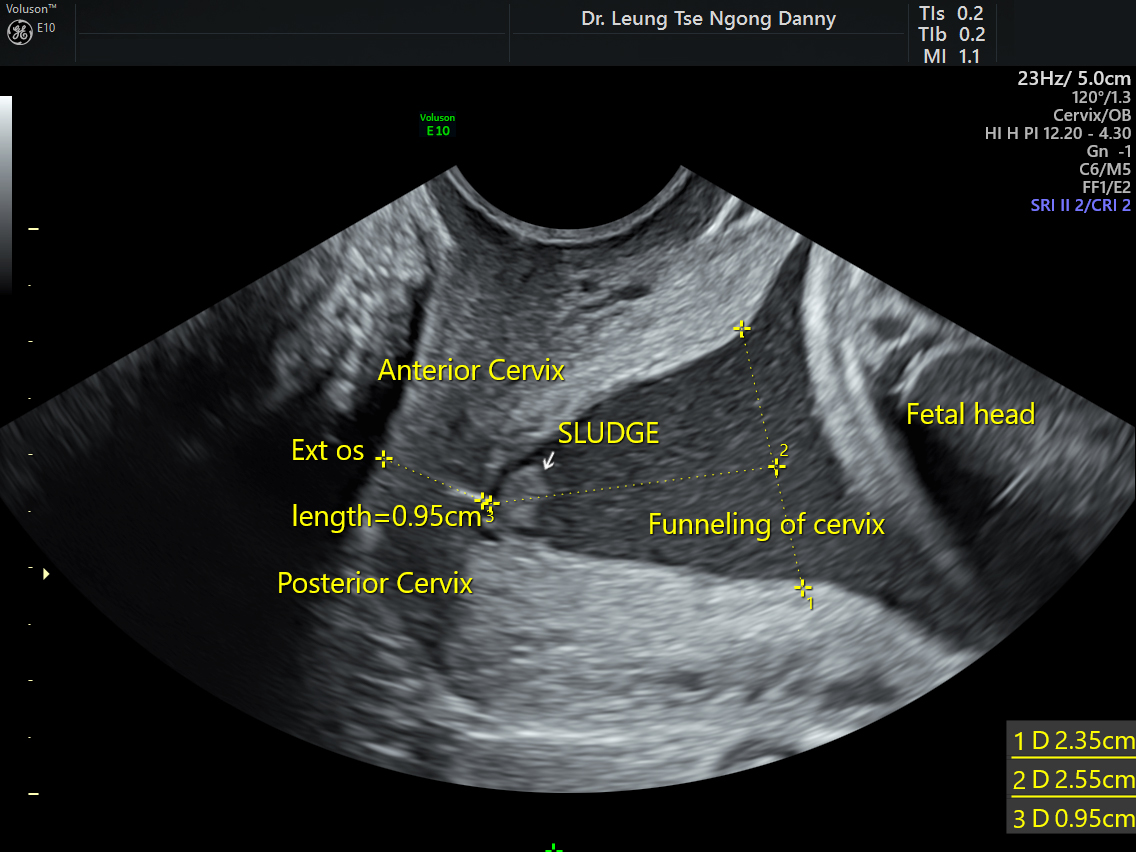
- Short cervix
- For women with a history of mid-trimester miscarriage or very early preterm birth but atypical for cervical incompetence, serial ultrasound measurements of the cervical length from 14-16 weeks onwards has been proposed. This can avoid unnecessarily intervention for those with long cervix. However, there are two pifalls with this approach:
- (i) Short cervix is a marker for preterm birth but may not be related to cervical incompetence. It is therefore unknown if the treatment for cervical incompetence can help those with short cervix;
- (ii) The shortening of the cervix can progress very rapidly. By the time the short cervix is found, significant cervical dilatation could have occurred and the treatment for cervical incompetence might be too late.
- Cerclage is a surgical procedure for occlusion of the cervix using sutures or synthetic tape. The mechanical reinforcement may increase the strength of the cervix. Also, the occlusion may help to prevent ascending infection from any bacteria in the vagina;
- It is usually performed at 14-16 weeks of gestation from transvaginal route. Very rarely, for those with a very deficient cervix, cerclage can be performed before pregnancy through the abdominal route by laparoscopic means;
- Multiple randomised controlled trials have been conducted to assess the efficacy of cervical cerclage in prevention of preterm birth. The data are hampered by the heterogeneity of recruited subjects (recruitment based on history, short cervix on one‐off ultrasound in high risk women, short cervix found by serial scans in high risk women, physical exam‐indicated, and short cervix found on scan in low risk or mixed populations, etc);
- For women with a typical history of cervical incompetence, most obstetricians will advise cervical cerclage at 14-16 weeks;
- For women with a history of preterm birth and a short cervix < 25mm, cervical cerclage has been shown to result in 40% reduction in preterm birth < 35 weeks of gestation. This reduction was not seen for women with a short cervix but no history of preterm birth in the past. So, for women with a history of mid-trimester miscarriage or early preterm birth but atypical of cervical incompetence, offer of cerclage when the cervical length is < 25 mm seems appropriate;
- The complications are uncommon but include infection, trauma to the bladder/ rectum and displacement of the stitch.
-

- Cervical length before cerclage

-

- Cervical length after cerclage

6. Arabin pessary
- It is a flexible silicone round cone-shaped device designed to occlude the cervix;
- Multiple randomised trials have been performed to assess the efficacy of the Arabin pessary and conflicting results have been reported;
- Of relevance to Hong Kong, a randomised study was published by the Chinese University of Hong Kong in 2012 on 108 patients with cervical length < 25mm between 20-24 weeks. The use of Arabin pessary was not found to reduce the incidence of preterm birth < 34 weeks of gestation compared with routine care;
- In a review published in May 2020, a list of all the randomised trials was presented and the conclusion was that the clinical efficacy has remained uncertain.
7. Vaginal progesterone
- Based on large randomised double-blinded placebo-controlled trials, the use of vaginal progesterone can significantly reduce the incidence of preterm birth < 34 weeks of gestation for women with short cervix on ultrasound at 20-22 weeks of gestation. It also appears to be a safe medication for the fetus.